
Articles
- Page Path
- HOME > Insights Cataract Refract Surg > Volume 11(1); 2026 > Article
-
Case Report
- Large incisional tear caused by abrupt Bell’s phenomenon during pocket irrigation in femtosecond laser-assisted small incision lenticule extraction
-
Sang Beom Han

-
Insights in Cataract and Refractive Surgery 2026;11(1):23-25.
DOI: https://doi.org/10.63375/icrs.25.015
Published online: February 26, 2026
Saevit Eye Hospital, Goyang, Korea
- Correspondence to: Sang Beom Han Saevit Eye Hospital, 1065 Jungang-ro, Ilsandong-gu, Goyang 10447, Korea Tel: +82-31-900-7700 E-mail: msbhan@saeviteye.com
• Received: December 22, 2025 • Revised: January 4, 2026 • Accepted: January 5, 2026
© 2026 Korean Society of Cataract and Refractive Surgery.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 530 Views
- 4 Download
Abstract
-
Purpose
- This study reports a case of a large incisional tear caused by abrupt Bell’s phenomenon during pocket irrigation in femtosecond laser-assisted small incision lenticule extraction (SMILE).
-
Case summary
- A 28-year-old male patient underwent SMILE surgery. During pocket irrigation of the right eye, Bell’s phenomenon suddenly occurred, resulting in a large inferior arcuate extension of the incision that reached the inferior cap margin. After confirming wound integrity and the absence of additional tissue damage, a bandage contact lens was applied. On postoperative day 7, the incision was self-sealed with intact wound integrity. Three months postoperatively, uncorrected distance visual acuity was 20/20 in both eyes. The right cornea remained stable, although a faint residual scar was observed at the site of the incisional tear.
-
Conclusion
- Abrupt eye movements during pocket irrigation in SMILE can cause large incisional tears. Surgeons should exercise heightened vigilance during irrigation, particularly in anxious or uncooperative patients, to prevent such complications.
Introduction
Case Report
Discussion
Article Information
Author contributions
All the work was done by SBH.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This paper was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (Grant No. NRF-2021R1F1A1048448).
Data availability
Not applicable.
Fig. 1.Still images from the intraoperative videos. (A) During pocket irrigation, a sudden upward ocular movement occurred due to Bell’s phenomenon in the right eye. (B) Following the abrupt movement, a large inferior arcuate extension of the incision (arrows) was observed.
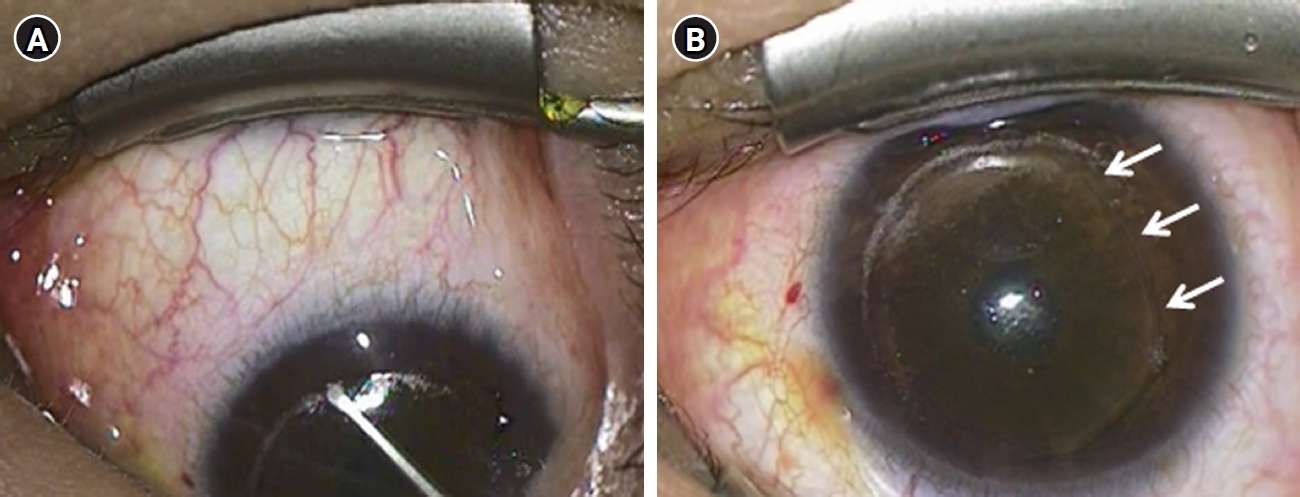
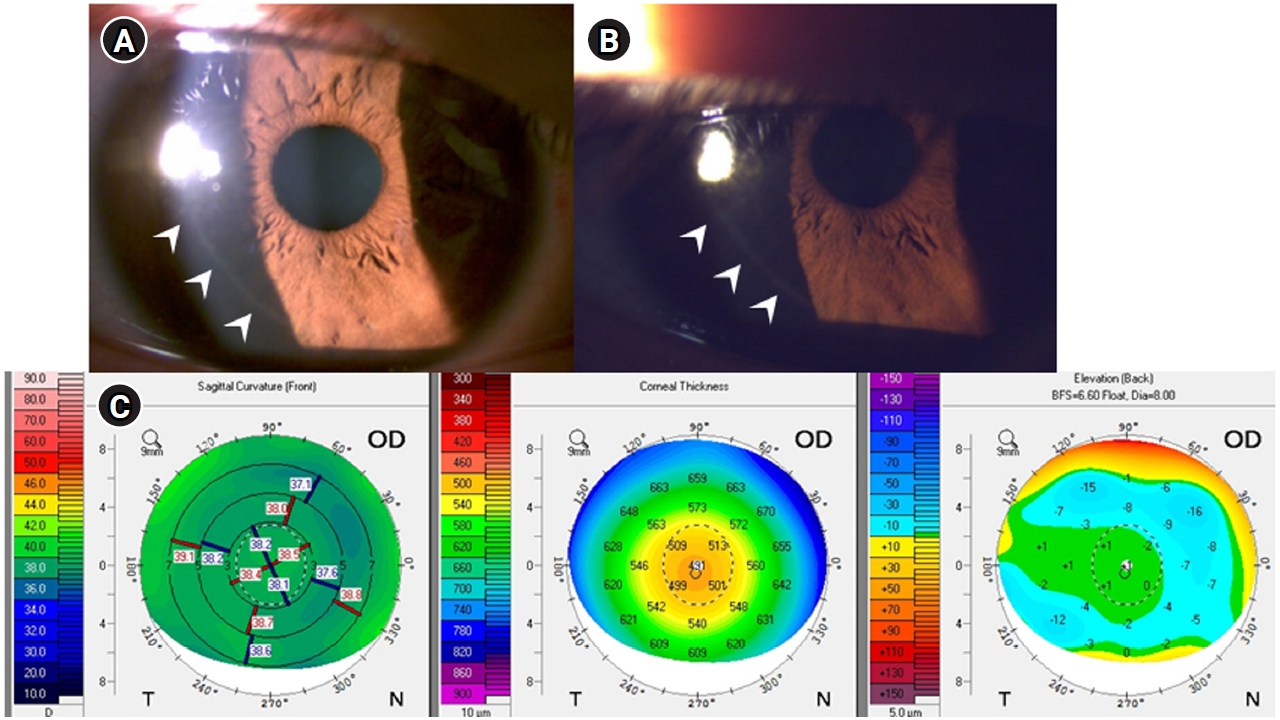
Fig. 2.Postoperative anterior segment photographs (A, B) and postoperative corneal topography (C). (A) An anterior segment photograph obtained on postoperative day 7 showed a self-sealed incision with intact wound integrity (arrowheads). (B) At 3 months postoperatively, a faint scar at the incisional tear site remained visible (arrowheads). (C) Postoperative corneal topography demonstrated no abnormal findings in the right eye (OD).
- 1. Hamed AM, Heikal MA, Soliman TT, et al. Smile intraoperative complications: incidence and management. Int J Ophthalmol 2019;12:280‒3. ArticlePubMedPMC
- 2. Asif MI, Bafna RK, Mehta JS, et al. Complications of small incision lenticule extraction. Indian J Ophthalmol 2020;68:2711‒22. ArticlePubMedPMC
- 3. Ivarsen A, Asp S, Hjortdal J. Safety and complications of more than 1500 small-incision lenticule extraction procedures. Ophthalmology 2014;121:822‒8. ArticlePubMed
- 4. Titiyal JS, Kaur M, Rathi A, et al. Learning curve of small incision lenticule extraction: challenges and complications. Cornea 2017;36:1377‒82. ArticlePubMed
- 5. Hamed AM, Abdelwahab SM, Soliman TT. Intraoperative complications of refractive small incision lenticule extraction in the early learning curve. Clin Ophthalmol 2018;12:665‒8. ArticlePubMedPMCPDF
References
Figure & Data
References
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteLarge incisional tear caused by abrupt Bell’s phenomenon during pocket irrigation in femtosecond laser-assisted small incision lenticule extraction

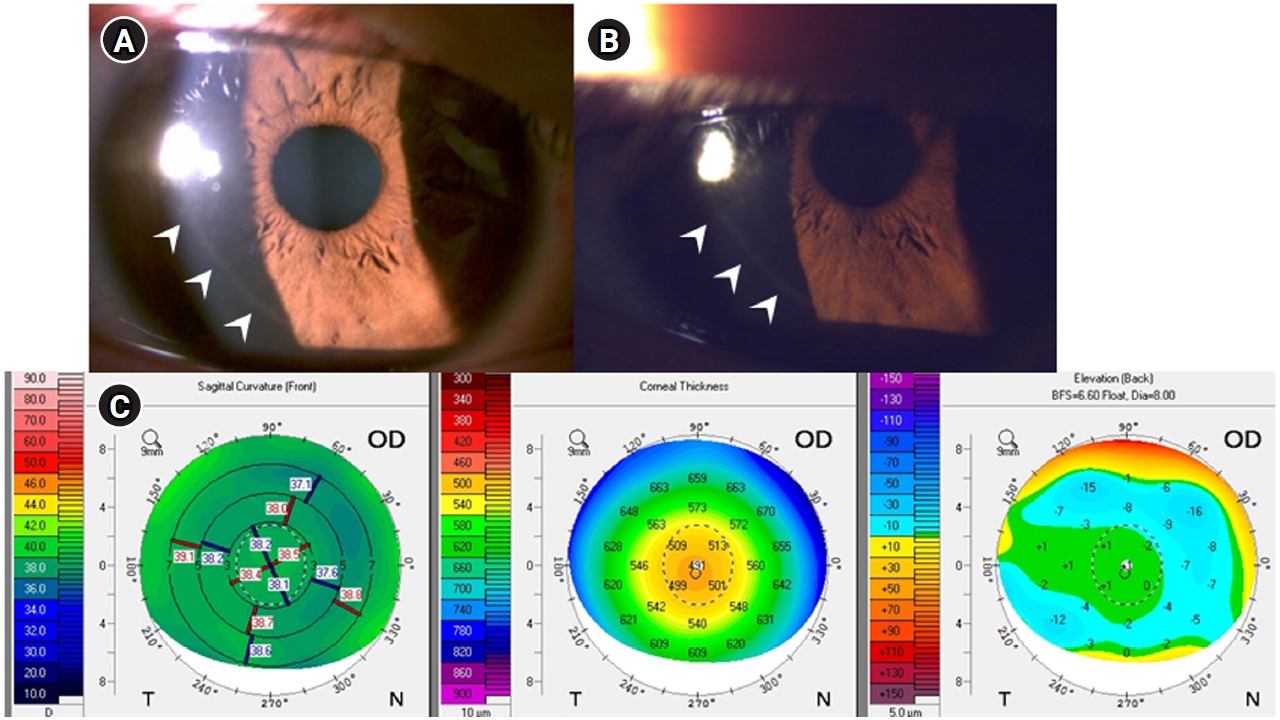
Fig. 1. Still images from the intraoperative videos. (A) During pocket irrigation, a sudden upward ocular movement occurred due to Bell’s phenomenon in the right eye. (B) Following the abrupt movement, a large inferior arcuate extension of the incision (arrows) was observed.
Fig. 2. Postoperative anterior segment photographs (A, B) and postoperative corneal topography (C). (A) An anterior segment photograph obtained on postoperative day 7 showed a self-sealed incision with intact wound integrity (arrowheads). (B) At 3 months postoperatively, a faint scar at the incisional tear site remained visible (arrowheads). (C) Postoperative corneal topography demonstrated no abnormal findings in the right eye (OD).
Fig. 1.
Fig. 2.
Large incisional tear caused by abrupt Bell’s phenomenon during pocket irrigation in femtosecond laser-assisted small incision lenticule extraction

