
Articles
- Page Path
- HOME > Insights Cataract Refract Surg > Volume 11(1); 2026 > Article
-
Original Article
- Therapeutic effects of diquafosol ophthalmic solution and carbomer eye gel in dry eye patients with lid wiper epitheliopathy
-
Jong Suk Song
 , In Ho Woo
, In Ho Woo -
Insights in Cataract and Refractive Surgery 2026;11(1):9-14.
DOI: https://doi.org/10.63375/icrs.25.019
Published online: February 26, 2026
1Department of Ophthalmology, Korea University College of Medicine, Seoul, Korea
- Correspondence to: Jong Suk Song Department of Ophthalmology, Korea University Guro Hospital, Korea University College of Medicine, 145 Anam-ro, Seongbuk-gu, Seoul 02841, Korea Tel: +82-2-2626-3178 E-mail: crisim@korea.ac.kr
• Received: December 31, 2025 • Revised: January 5, 2026 • Accepted: January 9, 2026
© 2026 Korean Society of Cataract and Refractive Surgery.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 919 Views
- 11 Download
Abstract
-
Purpose
- This study aimed to evaluate the therapeutic effects of 3% diquafosol tetrasodium ophthalmic solution (Diquas) and a carbomer-based, lipid-containing eye gel (Liposic, Bausch & Lomb) in dry eye patients with lid wiper epitheliopathy (LWE) that was refractory to topical treatment with conventional artificial tears.
-
Methods
- Thirty-three dry eye patients with LWE of the upper eyelid were treated with 3% diquafosol ophthalmic solution administered six times daily and a carbomer-based, lipid-containing eye gel administered four times daily. After the 2-week treatment period, changes in ocular symptoms were assessed using a visual analog scale (VAS), and changes in ocular signs were evaluated using tear film break-up time (TBUT), corneal staining, and LWE grading.
-
Results
- The mean patient age was 37.58±12.35 years (range, 21–67 years); six patients were male and 27 were female. At baseline, the mean VAS symptom score was 7.18±1.47, and the mean TBUT was 2.78±0.78 seconds. After 2 weeks of treatment, the mean VAS score decreased to 4.87±1.97, and the mean TBUT increased to 3.68±1.08 seconds (both P<0.05). The mean corneal staining score was 1.09±1.50, and the mean LWE grade was 5.76±0.61 at baseline. Following treatment, these values decreased to 0.55±0.83 and 2.24±1.95, respectively (both P<0.05). Among the objective parameters, only the LWE grade showed a significant correlation with the VAS score.
-
Conclusion
- The LWE grade showed a significant correlation with ocular symptoms. Combined treatment with diquafosol ophthalmic solution and a carbomer-based, lipid-containing eye gel demonstrated excellent therapeutic effects in dry eye patients with LWE who were refractory to treatment with conventional artificial tears.
Introduction
Methods
Results
Discussion
Article Information
Author contributions
Conceptualization: JSS. Formal analysis: JSS. Investigation: JSS. Methodology: IHW. Supervision: JSS. Writing - original draft: IHW. Writing - review & editing: JSS. Final approval of the manuscript: all authors.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) and funded by the Ministry of Education (NRF-2017R1D1A1B03028552). The funding organization had no role in the design or conduct of this research.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Fig. 1.A 35-year-old female patient. Slit-lamp examination performed using a yellow filter and maximal cobalt blue illumination with fluorescein staining demonstrated lid wiper staining (A) and a clear corneal state (B). After 2 weeks of topical treatment with Diquas and Liposic, lid wiper staining was markedly improved (C), and the corneal state remained clear (D).
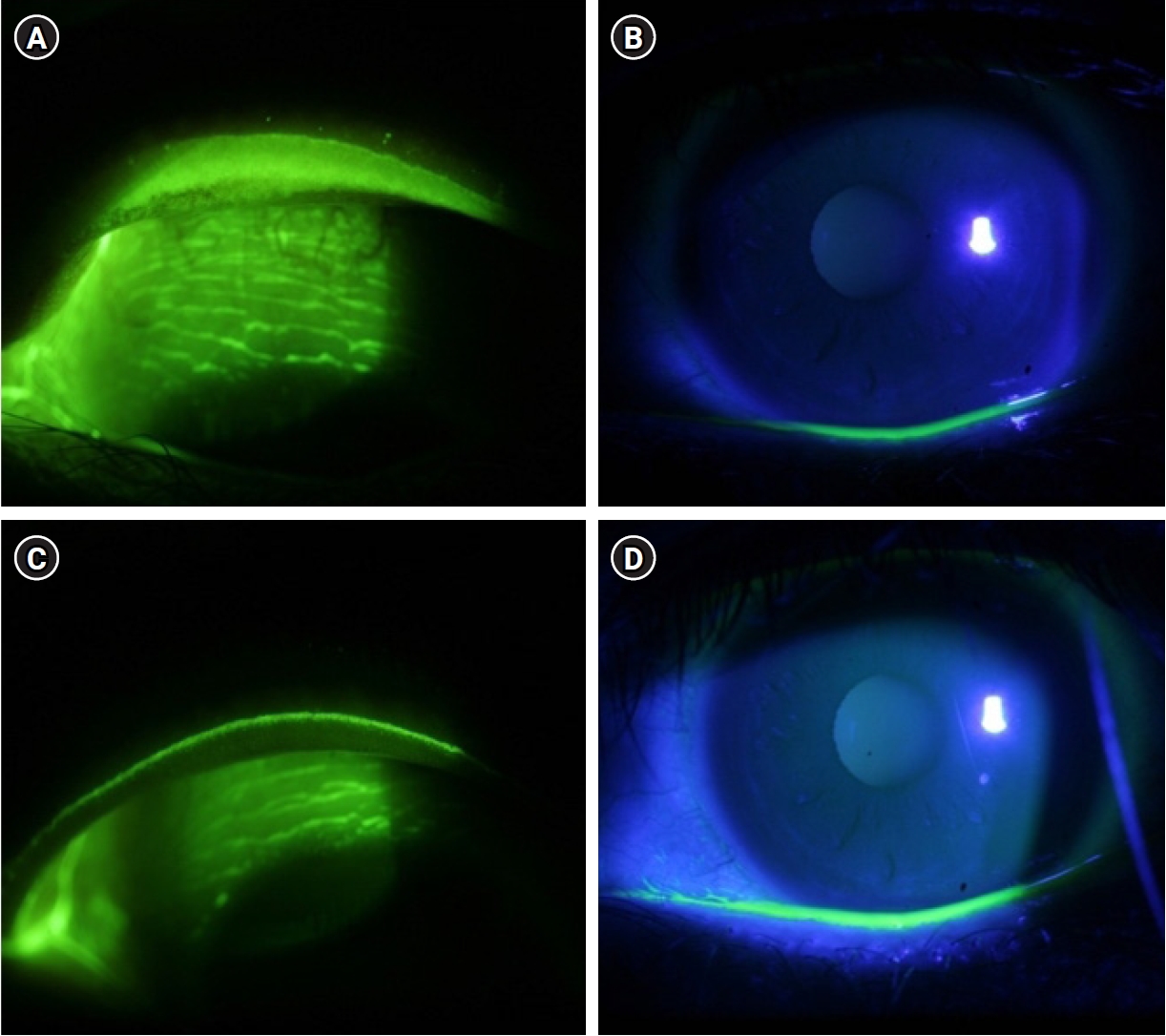
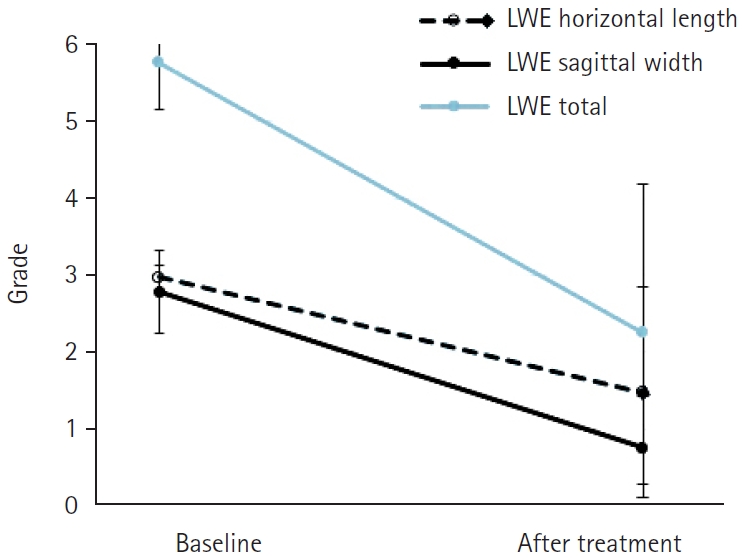
Table 1.Patient demographics
Table 2.Changes in dry eye parameters after treatment
Table 3.Correlations between parameters before treatment
| Parameter | Age | LWE | VAS | Corneal staining | TBUT |
|---|---|---|---|---|---|
| Age | - | ||||
| LWE | 0.159 | - | |||
| VAS | –0.143 | 0.482* | - | ||
| Corneal staining | 0.395* | 0.126 | 0.105 | - | |
| TBUT | –0.460* | –0.241 | –0.183 | –0.408* | - |
Table 4.Correlations between parameters after treatment
| Parameter | Age | LWE | VAS | Corneal staining | TBUT |
|---|---|---|---|---|---|
| Age | - | ||||
| LWE | –0.099 | - | |||
| VAS | –0.047 | 0.364* | - | ||
| Corneal staining | 0.090 | 0.301 | 0.117 | - | |
| TBUT | –0.050 | –0.337 | –0.251 | –0.389* | - |
- 1. Korb DR, Greiner JV, Herman JP, et al. Lid-wiper epitheliopathy and dry-eye symptoms in contact lens wearers. CLAO J 2002;28:211‒6. ArticlePubMed
- 2. Korb DR, Herman JP, Greiner JV, et al. Lid wiper epitheliopathy and dry eye symptoms. Eye Contact Lens 2005;31:2‒8. ArticlePubMed
- 3. Korb DR, Herman JP, Finnemore VM, et al. An evaluation of the efficacy of fluorescein, rose bengal, lissamine green, and a new dye mixture for ocular surface staining. Eye Contact Lens 2008;34:61‒4. ArticlePubMed
- 4. Korb DR, Herman JP, Blackie CA, et al. Prevalence of lid wiper epitheliopathy in subjects with dry eye signs and symptoms. Cornea 2010;29:377‒83. ArticlePubMed
- 5. Willcox MD, Argueso P, Georgiev GA, et al. TfOS DEWS II tear film report. Ocul Surf 2017;15:366‒403. ArticlePubMedPMC
- 6. Yamamoto Y, Shiraishi A, Sakane Y, et al. Involvement of eyelid pressure in lid-wiper epitheliopathy. Curr Eye Res 2016;41:171‒8. ArticlePubMed
- 7. Berry M, Pult H, Purslow C, Murphy PJ. Mucins and ocular signs in symptomatic and asymptomatic contact lens wear. Optom Vis Sci 2008;85:E930‒8. ArticlePubMed
- 8. Pult H, Purslow C, Murphy PJ. The relationship between clinical signs and dry eye symptoms. Eye (Lond) 2011;25:502‒10. ArticlePubMedPMCPDF
- 9. Wolffsohn JS, Arita R, Chalmers R, et al. TfOS DEWS II diagnostic methodology report. Ocul Surf 2017;15:539‒74. ArticlePubMed
- 10. Eom Y, Lee JS, Lee HK, et al. Comparison of conjunctival staining between lissamine green and yellow filtered fluorescein sodium. Can J Ophthalmol 2015;50:273‒7. ArticlePubMed
- 11. Lemp MA. Report of the National Eye Institute/Industry workshop on clinical trials in dry eyes. CLAO J 1995;21:221‒32. PubMed
- 12. Fujihara T, Murakami T, Nagano T, et al. INS365 suppresses loss of corneal epithelial integrity by secretion of mucin-like glycoprotein in a rabbit short-term dry eye model. J Ocul Pharmacol Ther 2002;18:363‒70. ArticlePubMed
- 13. Matsumoto Y, Ohashi Y, Watanabe H, Tsubota K. Efficacy and safety of diquafosol ophthalmic solution in patients with dry eye syndrome: a Japanese phase 2 clinical trial. Ophthalmology 2012;119:1954‒60. ArticlePubMed
- 14. Tauber J, Davitt WF, Bokosky JE, et al. Double-masked, placebo-controlled safety and efficacy trial of diquafosol tetrasodium (INS365) ophthalmic solution for the treatment of dry eye. Cornea 2004;23:784‒92. ArticlePubMed
- 15. Nakamura M, Imanaka T, Sakamoto A. Diquafosol ophthalmic solution for dry eye treatment. Adv Ther 2012;29:579‒89. ArticlePDF
- 16. Marner K, Mooller PM, Dillon M, Rask-Pedersen E. Viscous carbomer eye drops in patients with dry eyes: efficacy and safety: a randomized, open, cross-over, multicentre study. Acta Ophthalmol Scand 1996;74:249‒52. PubMed
- 17. Chung SH, Lim SA, Tchach H. Efficacy and safety of carbomer-based lipid-containing artificial tear formulations in patients with dry eye syndrome. Cornea 2016;35:181‒6. ArticlePubMed
- 18. Yeniad B, Beginoglu M, Bilgin LK. Lid-wiper epitheliopathy in contact lens users and patients with dry eye. Eye Contact Lens 2010;36:140‒3. ArticlePubMed
- 19. Gipson IK. Distribution of mucins at the ocular surface. Exp Eye Res 2004;78:379‒88. ArticlePubMed
- 20. Fahmy AM, Hardten DR. Treating ocular surface disease: new agents in development. Clin Ophthalmol 2011;5:465‒72. ArticlePubMedPMC
- 21. Takaoka-Shichijo Y, Sakamoto A, Nakamura M. Effect of diquafosol tetrasodium on MUC5AC secretion by rabbit conjunctival tissues. Eye 2011;28:261‒5.
- 22. Yuko S, Masatsugu N. Stimulatory effect of diquafosol tetrasodium on the expression of membrane-binding mucin genes in cultured human corneal epithelial cells. J Eye 2011;28:425‒9.
- 23. Guthrie SE, Jones L, Blackie CA, Korb DR. A comparative study between an oil-in-water emulsion and nonlipid eye drops used for rewetting contact lenses. Eye Contact Lens 2015;41:373‒7. ArticlePubMed
- 24. Ngo W, Srinivasan S, Houtman D, Jones L. The relief of dry eye signs and symptoms using a combination of lubricants, lid hygiene and ocular nutraceuticals. J Optom 2017;10:26‒33. ArticlePubMedPMC
- 25. Itakura H, Kashima T, Itakura M, et al. Topical rebamipide improves lid wiper epitheliopathy. Clin Ophthalmol 2013;7:2137‒41. ArticlePubMedPMC
- 26. Efron N, Brennan NA, Morgan PB, Wilson T. Lid wiper epitheliopathy. Prog Retin Eye Res 2016;53:140‒74. ArticlePubMed
References
Figure & Data
References
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteTherapeutic effects of diquafosol ophthalmic solution and carbomer eye gel in dry eye patients with lid wiper epitheliopathy

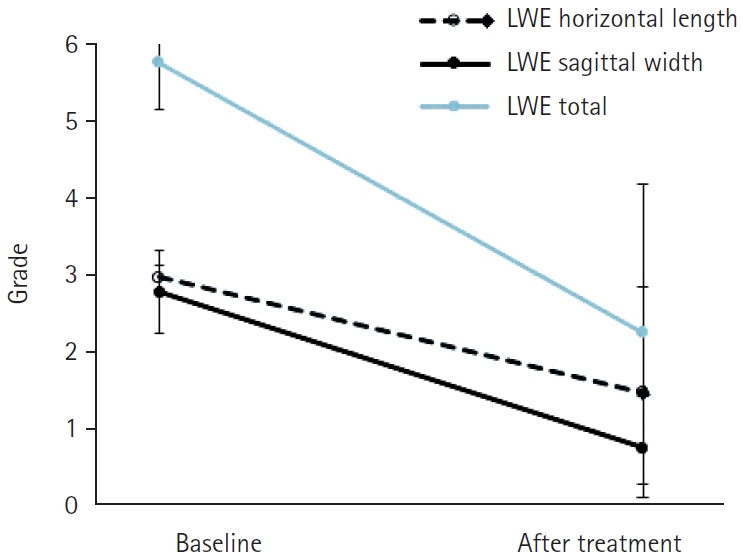
Fig. 1. A 35-year-old female patient. Slit-lamp examination performed using a yellow filter and maximal cobalt blue illumination with fluorescein staining demonstrated lid wiper staining (A) and a clear corneal state (B). After 2 weeks of topical treatment with Diquas and Liposic, lid wiper staining was markedly improved (C), and the corneal state remained clear (D).
Fig. 2. Graphs illustrating lid wiper epitheliopathy (LWE) grade before and after treatment.
Fig. 1.
Fig. 2.
Therapeutic effects of diquafosol ophthalmic solution and carbomer eye gel in dry eye patients with lid wiper epitheliopathy
| Characteristic | Value |
|---|---|
| Age (yr) | 37.58±12.35 |
| Sex (male:female) | 6:27 |
| Lid wiper epitheliopathy (grade) | |
| Horizontal length | 2.97±0.17 |
| Sagittal width | 2.79±0.54 |
| Total | 5.76±0.61 |
| Visual analog scale (score) | 7.18±1.47 |
| Corneal staining (score) | 1.09±1.50 |
| Tear film break-up time (sec) | 2.78±0.78 |
| Parameter | Baseline | After treatment | P-value |
|---|---|---|---|
| Lid wiper epitheliopathy | |||
| Horizontal length | 2.97±0.17 | 1.48±1.37 | <0.001 |
| Sagittal width | 2.79±0.54 | 0.76±0.66 | <0.001 |
| Total | 5.76±0.61 | 2.24±1.95 | <0.001 |
| Visual analog scale (score) | 7.18±1.47 | 4.87±1.97 | <0.001 |
| Corneal staining (score) | 1.09±1.50 | 0.55±0.83 | 0.024 |
| Tear film break-up time (sec) | 2.78±0.78 | 3.68±1.08 | <0.001 |
| Parameter | Age | LWE | VAS | Corneal staining | TBUT |
|---|---|---|---|---|---|
| Age | - | ||||
| LWE | 0.159 | - | |||
| VAS | –0.143 | 0.482 |
- | ||
| Corneal staining | 0.395 |
0.126 | 0.105 | - | |
| TBUT | –0.460 |
–0.241 | –0.183 | –0.408 |
- |
| Parameter | Age | LWE | VAS | Corneal staining | TBUT |
|---|---|---|---|---|---|
| Age | - | ||||
| LWE | –0.099 | - | |||
| VAS | –0.047 | 0.364 |
- | ||
| Corneal staining | 0.090 | 0.301 | 0.117 | - | |
| TBUT | –0.050 | –0.337 | –0.251 | –0.389 |
- |
Table 1. Patient demographics
Values are presented as mean±standard deviation.
Table 2. Changes in dry eye parameters after treatment
Values are presented as mean±standard deviation.
Table 3. Correlations between parameters before treatment
LWE, lid wiper epitheliopathy; VAS, visual analog scale; TBUT, tear film break-up time. Statistically significant P-value <0.05 in Pearson correlation analysis.
Table 4. Correlations between parameters after treatment
LWE, lid wiper epitheliopathy; VAS, visual analog scale; TBUT, tear film break-up time. Statistically significant P-value <0.05 in Pearson correlation analysis.

