
Articles
- Page Path
- HOME > Insights Cataract Refract Surg > Volume 10(2); 2025 > Article
-
Case Report
- Diffuse lamellar keratitis after small incision lenticule extraction: presumably related to meibomian gland dysfunction
-
Sang Beom Han

-
Insights in Cataract and Refractive Surgery 2025;10(2):61-64.
DOI: https://doi.org/10.63375/icrs.25.008
Published online: June 30, 2025
Saevit Eye Hospital, Goyang, Korea
- Correspondence to: Sang Beom Han Saevit Eye Hospital, 1065 Jungang-ro, Ilsandong-gu, Goyang 10447, Korea Tel: +82-31-900-7700 E-mail: msbhan@saeviteye.com
• Received: April 9, 2025 • Revised: May 20, 2025 • Accepted: May 20, 2025
© 2025 Korean Society of Cataract and Refractive Surgery.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,296 Views
- 28 Download
Abstract
-
Purpose
- This report presents a case of diffuse lamellar keratitis (DLK) after femtosecond laser-assisted small incision lenticule extraction (SMILE). The case was presumably associated with meibomian gland dysfunction (MGD).
-
Case summary
- A 25-year-old male patient underwent SMILE surgery. Preoperative examination revealed MGD in both eyes. Despite vigorous cleaning of the eyelid margin and irrigation of the ocular surface, meibomian gland secretion floating on the ocular surface was observed after the lenticule extraction in the right eye. At 2 days postoperatively, stage I DLK was detected. After aggressive topical steroid treatment, the DLK completely resolved without any sequalae.
-
Conclusion
- DLK can occur in association with MGD. Attention should be paid when performing SMILE in eyes with MGD.
Introduction
Case Report
Discussion
Article Information
Author contributions
All the work was done by SBH.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This paper was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (Grant No. NRF-2021R1F1A1048448).
Data availability
Not applicable.
Fig. 1.Still images of the intraoperative videos. (A) Meibomian gland secretion (arrows) floating on the ocular surface was detected after the lenticule extraction in the right eye. (B) Meibomian gland secretion (arrows) on the upper eyelid was visible in the left eye during lenticule separation.
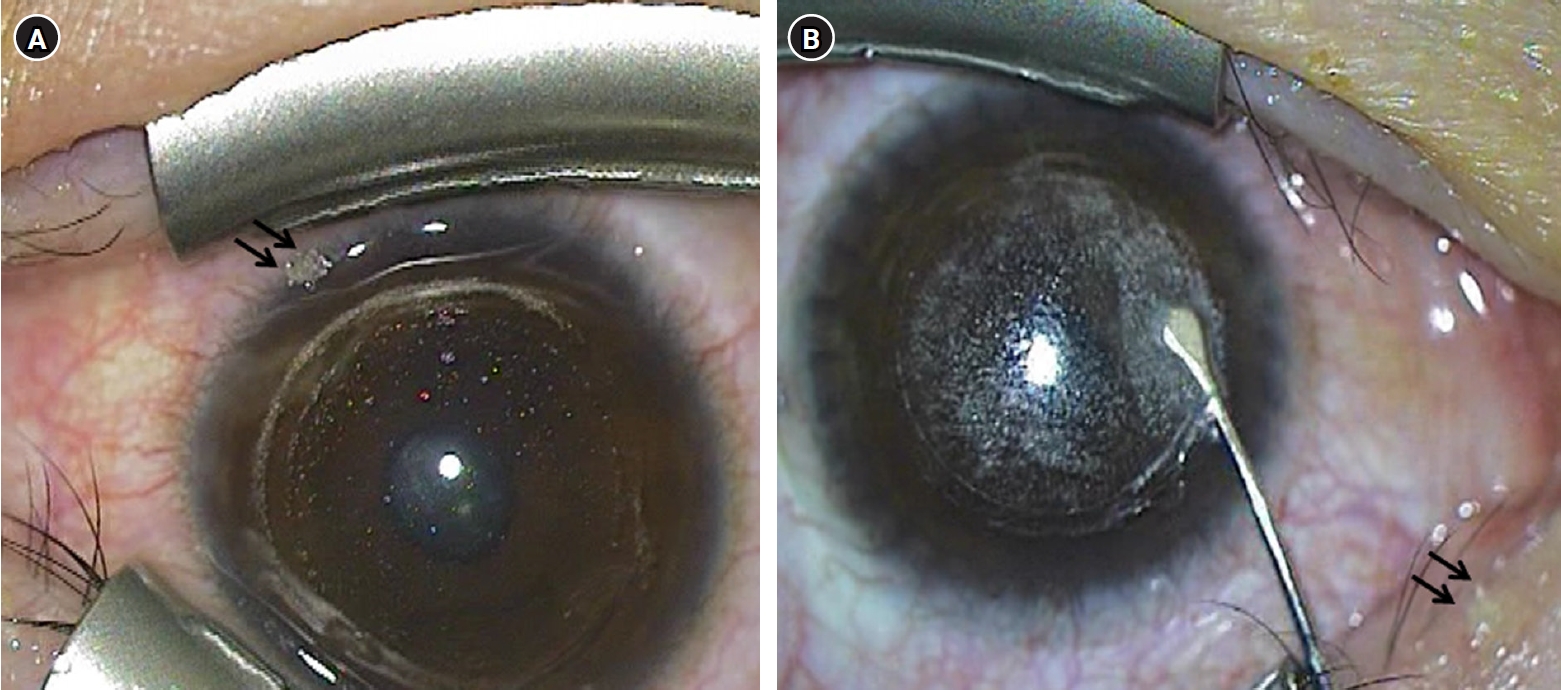
Fig. 2.Anterior segment photographs at the second day after surgery. (A, B) Stage I diffuse lamellar keratitis with multiple granular infiltrates (arrows) was observed at the interface in the right eye.
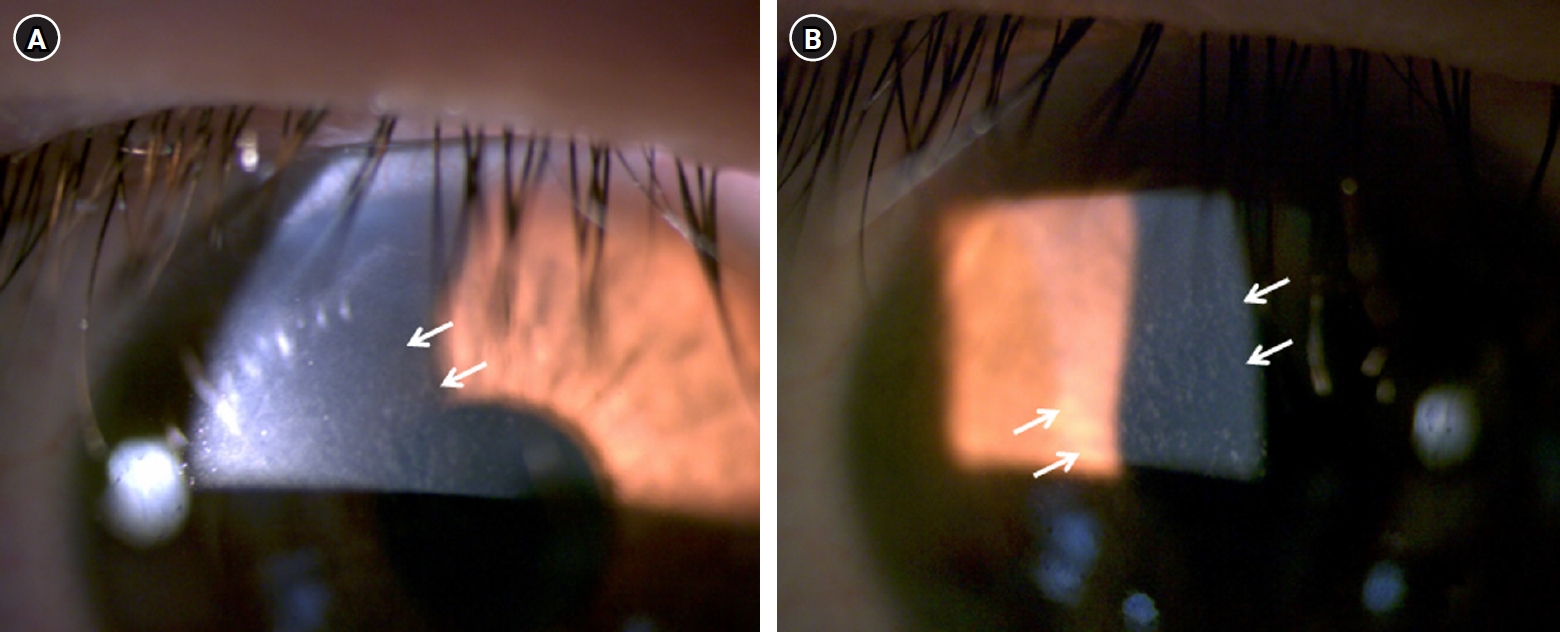
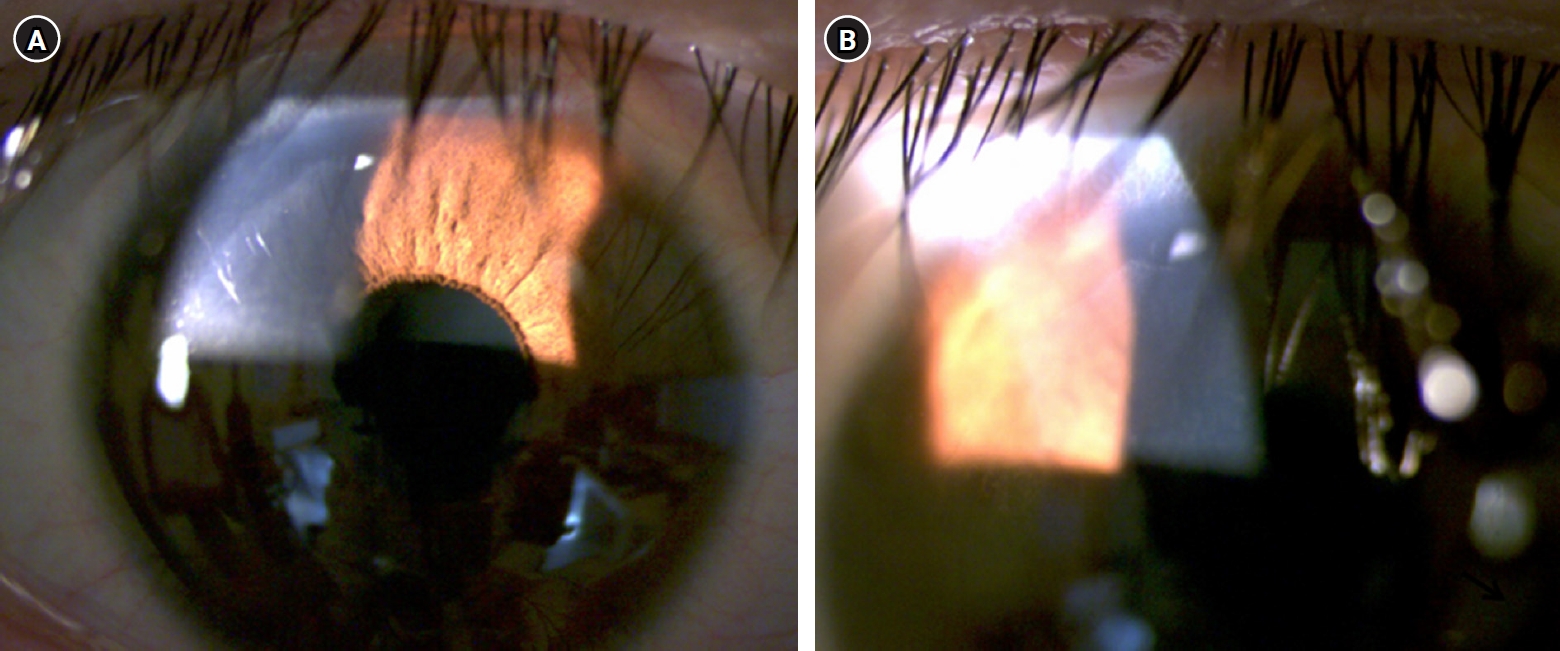
Fig. 3.Anterior segment photographs at the fifth day after surgery. (A, B) Improvement in diffuse lamellar keratitis can be observed at the corneal interface.
- 1. Smith RJ, Maloney RK. Diffuse lamellar keratitis: a new syndrome in lamellar refractive surgery. Ophthalmology 1998;105:1721‒6. ArticlePubMed
- 2. Kymionis GD, Tsoulnaras KI, Tsakalis NG, Grentzelos MA. Diffuse lamellar keratitis in the femtosecond-assisted LASIK flap tunnel. Clin Ophthalmol 2014;8:1065‒7. ArticlePubMedPMC
- 3. Linebarger EJ, Hardten DR, Lindstrom RL. Diffuse lamellar keratitis: diagnosis and management. J Cataract Refract Surg 2000;26:1072‒7. ArticlePubMed
- 4. Labani S, Basli E, Goemaere I, et al. Atypical severe diffuse lamellar keratitis presenting as concentric rings after femtosecond laser-assisted small-incision lenticule extraction (SMILE). J Fr Ophtalmol 2020;43:e95‒9. ArticlePubMed
- 5. Wilson SE, de Oliveira RC. Pathophysiology and treatment of diffuse lamellar keratitis. J Refract Surg 2020;36:124‒30. ArticlePubMed
- 6. Yuan M, Ji R, Zhang R. A case of severe diffuse lamellar keratitis after small-incision lenticule extraction operation. Indian J Ophthalmol 2024;72:1219‒23. ArticlePubMedPMC
- 7. Alqahtani SS. A case report of diffuse lamellar keratitis after femtoSMILE refractive surgery. Case Rep Ophthalmol 2020;11:582‒7. ArticlePubMedPMCPDF
- 8. Ambrósio R Jr, Periman LM, Netto MV, Wilson SE. Bilateral marginal sterile infiltrates and diffuse lamellar keratitis after laser in situ keratomileusis. J Refract Surg 2003;19:154‒8. ArticlePubMed
- 9. Balestrazzi A, Balestrazzi A, Giannico MI, et al. Diagnosis, clinical trend, and treatment of diffuse lamellar keratitis after femtosecond laser-assisted in situ keratomileusis: a case report. Case Rep Ophthalmol 2018;9:457‒64. ArticlePubMedPMCPDF
- 10. Fogla R, Rao SK, Padmanabhan P. Diffuse lamellar keratitis: are meibomian secretions responsible? J Cataract Refract Surg 2001;27:493‒5. ArticlePubMed
- 11. Zhao J, He L, Yao P, et al. Diffuse lamellar keratitis after small-incision lenticule extraction. J Cataract Refract Surg 2015;41:400‒7. ArticlePubMed
- 12. Reinstein DZ, Stuart AJ, Vida RS, et al. Incidence and outcomes of sterile multifocal inflammatory keratitis and diffuse lamellar keratitis after SMILE. J Refract Surg 2018;34:751‒9. ArticlePubMed
- 13. Wang Y, Ma J, Zhang L, et al. Postoperative corneal complications in small incision lenticule extraction: long-term study. J Refract Surg 2019;35:146‒52. ArticlePubMed
- 14. Suzuki T. Inflamed obstructive meibomian gland dysfunction causes ocular surface inflammation. Invest Ophthalmol Vis Sci 2018;59:DES94‒101. ArticlePubMed
- 15. Moshirfar M, Zhang S, Pandya S, et al. Incidence and Management of epithelial-related complications after SMILE. Clin Ophthalmol 2023;17:2777‒89. ArticlePubMedPMCPDF
References
Figure & Data
References
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteDiffuse lamellar keratitis after small incision lenticule extraction: presumably related to meibomian gland dysfunction
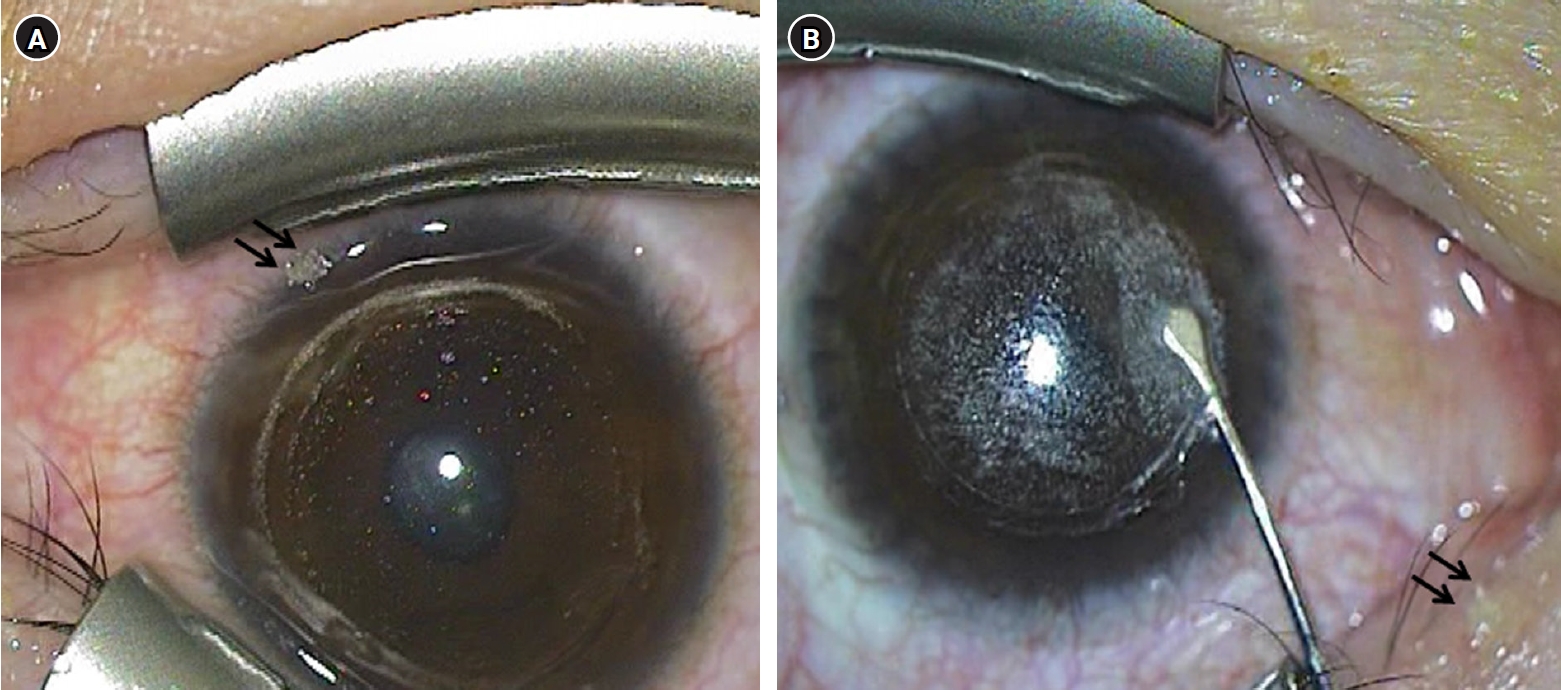
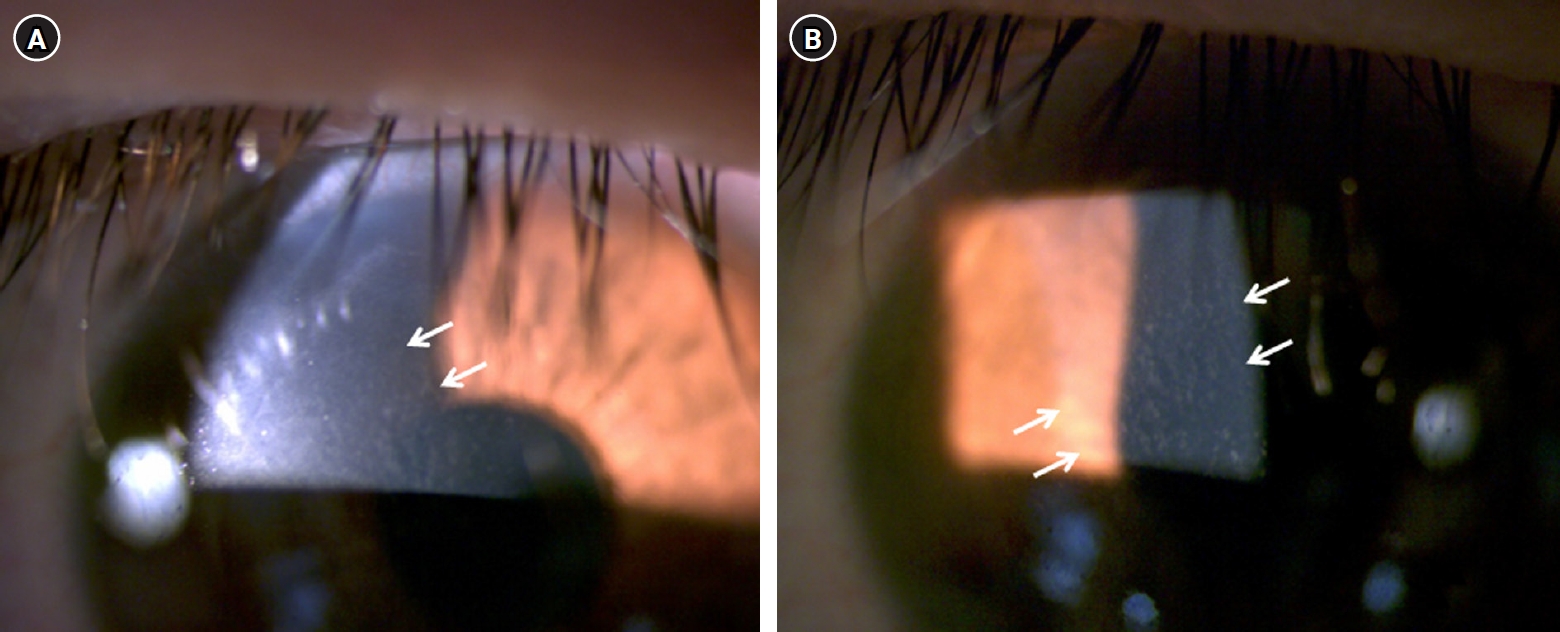
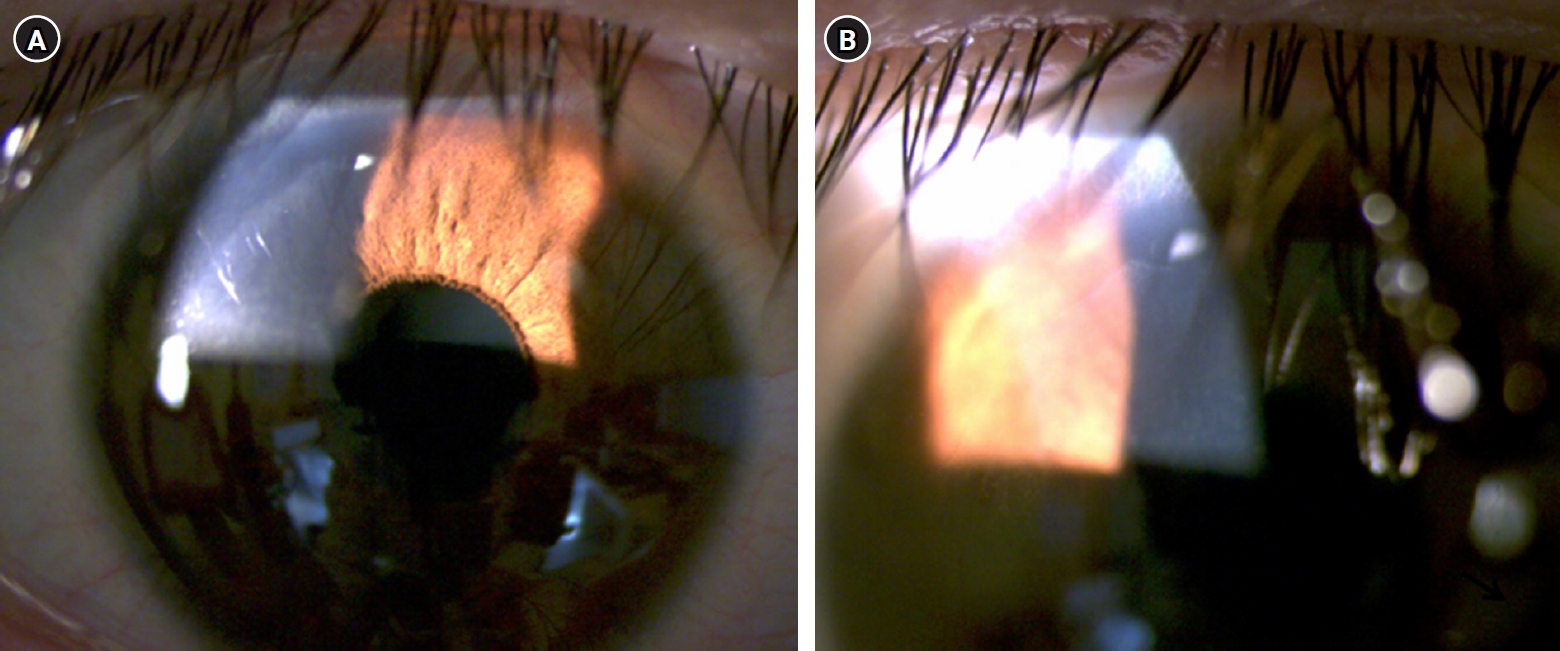
Fig. 1. Still images of the intraoperative videos. (A) Meibomian gland secretion (arrows) floating on the ocular surface was detected after the lenticule extraction in the right eye. (B) Meibomian gland secretion (arrows) on the upper eyelid was visible in the left eye during lenticule separation.
Fig. 2. Anterior segment photographs at the second day after surgery. (A, B) Stage I diffuse lamellar keratitis with multiple granular infiltrates (arrows) was observed at the interface in the right eye.
Fig. 3. Anterior segment photographs at the fifth day after surgery. (A, B) Improvement in diffuse lamellar keratitis can be observed at the corneal interface.
Fig. 1.
Fig. 2.
Fig. 3.
Diffuse lamellar keratitis after small incision lenticule extraction: presumably related to meibomian gland dysfunction

