
Articles
- Page Path
- HOME > Insights Cataract Refract Surg > Volume 10(2); 2025 > Article
-
Original Article
망막질환이 있는 환자에서 연속초점 인공수정체와 강화단초점 인공수정체 및 단초점 인공수정체의 효과 -
김은철

-
Efficacy of extended depth of focus, enhanced monofocal, and monofocal intraocular lenses in patients with retinal disease -
Eun Chul Kim
-
Insights in Cataract and Refractive Surgery 2025;10(2):52-60.
DOI: https://doi.org/10.63375/icrs.25.009
Published online: June 30, 2025
가톨릭대학교 의과대학 부천성모병원 안과학교실
Department of Ophthalmology, Bucheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Bucheon, Korea
- Correspondence to: Eun Chul Kim Department of Ophthalmology, The Catholic University of Korea, Bucheon St. Mary's Hospital, 327 Sosa-ro, Wonmi-gu, Bucheon 14647, Korea Tel: +82-32-340-2125 E-mail: eunchol@hanmail.net
• Received: April 15, 2025 • Revised: June 12, 2025 • Accepted: June 12, 2025
© 2025 Korean Society of Cataract and Refractive Surgery.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,558 Views
- 21 Download
국문초록
-
목적
- 망막질환이 있는 백내장 환자에서 연속초점 인공수정체와 강화단초점 인공수정체와 단초점 인공수정체의 임상 결과를 비교하고자 한다.
-
방법
- 본 연구는 강화단초점 인공수정체(TECNIS Eyhance: ICB00) 36안(1군), 연속초점 인공수정체(TECNIS Symfony: ZXR00) 36안(2군), 단초점 인공수정체(TECNIS Monofocal: ZCB00) 31안(3군)을 대상으로 후향적으로 시행되었다. 술 후 2개월 나안과 교정 원거리, 중간거리, 근거리 시력과 현성굴절검사 및 환자 만족도 설문을 시행하였다.
-
결과
- 수술 후 나안과 교정 원거리 시력과 현성굴절검사 결과는 세 군 모두 수술 전보다 개선되었다(P<0.05). 그러나 나안 중간거리 시력은 1군(0.13±0.12 logMAR)과 2군(0.10±0.11)이 3군(0.25±0.15)보다 유의하게 우수하였다(P<0.05). 나안 근거리 시력은 2군(0.18±0.12 logMAR)이 1군(0.32±0.20)과 3군(0.45±0.26)보다 유의하게 우수하였다(P<0.05). 세 군에서 황반부종과 황반원공을 가진 환자는 망막전막과 고도근시환자에 비해 원거리 나안시력이 유의하지 않지만 낮았다. 전체적인 시력의 만족도는 1군(1.58±0.81)과 2군(1.46±0.75)이 3군(1.83±0.97)보다 유의하게 높았다(P<0.05).
-
결론
- 망막질환이 있는 환자에서 연속초점 인공수정체와 강화단초점 인공수정체는 중간거리 시력과 근거리 시력이 단초점 인공수정체보다 더 나았다. 황반부종과 황반원공을 가진 환자는 망막전막과 고도근시환자에 비해 단초점 인공수정체 삽입이 권장된다.
Abstract
-
Purpose
- The aim of this study was to compare the visual quality of extended depth of focus (EDOF), enhanced monofocal, and monofocal intraocular lenses (IOLs) in patients with retinal disease.
-
Methods
- In total, 103 eyes from 93 patients (group 1: enhanced monofocal ICB00, n=36; group 2: EDOF ZXR00, n=36; group 3: monofocal ZCB00, n=31) were retrospectively enrolled. Uncorrected and corrected near visual acuity (UNVA, CNVA), intermediate visual acuity (UIVA, CIVA), and distance visual acuity (UDVA, CDVA), manifest refraction spherical equivalent (MRSE), and satisfaction scores were assessed before and after surgery.
-
Results
- The postoperative UDVA, CDVA, and MRSE of the three groups were better than the preoperative data, respectively (P<0.05). The UIVA of group 1 (0.13±0.12 logMAR) and 2 (0.10±0.11) was significantly better than that of groups 3 (0.25±0.15) (P<0.05). The UNVA of group 2 (0.18±0.12) was significantly better than that of groups 1 (0.32±0.20) and 3 (0.45±0.26; P<0.05). The UDVA of patients with macular edema and macular holes was insignificantly lower than that of epiretinal membranes and high myopia. The overall satisfaction of group 1 (1.58±0.81) and 2 (1.46±0.75) was significantly better than that of groups 3 (1.83±0.97; P<0.05).
-
Conclusion
- EDOF and enhanced monofocal IOLs were associated with better intermediate and near vision than monofocal IOLs in patients with retinal disease. However, monofocal IOLs are recommended in patients with macular edema and macular holes, unlike patients with epiretinal membranes and high myopia.
서론
방법
결과
고찰
Article Information
Author contributions
All the work was done by ECK.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
Not applicable.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Fig. 1.Postoperative uncorrected distance visual acuity (UDVA) in patients with retinal disease who were treated using the three intraocular lenses. The postoperative UDVA values in the three groups were better than the preoperative values, respectively (P<0.05). However, there was no statistically significant difference in postoperative UDVA among the three groups. Group 1: enhanced monofocal ICB00, n=36; Group 2: extended depth of focus ZXR00, n=36; Group 3: monofocal ZCB00, n=31.
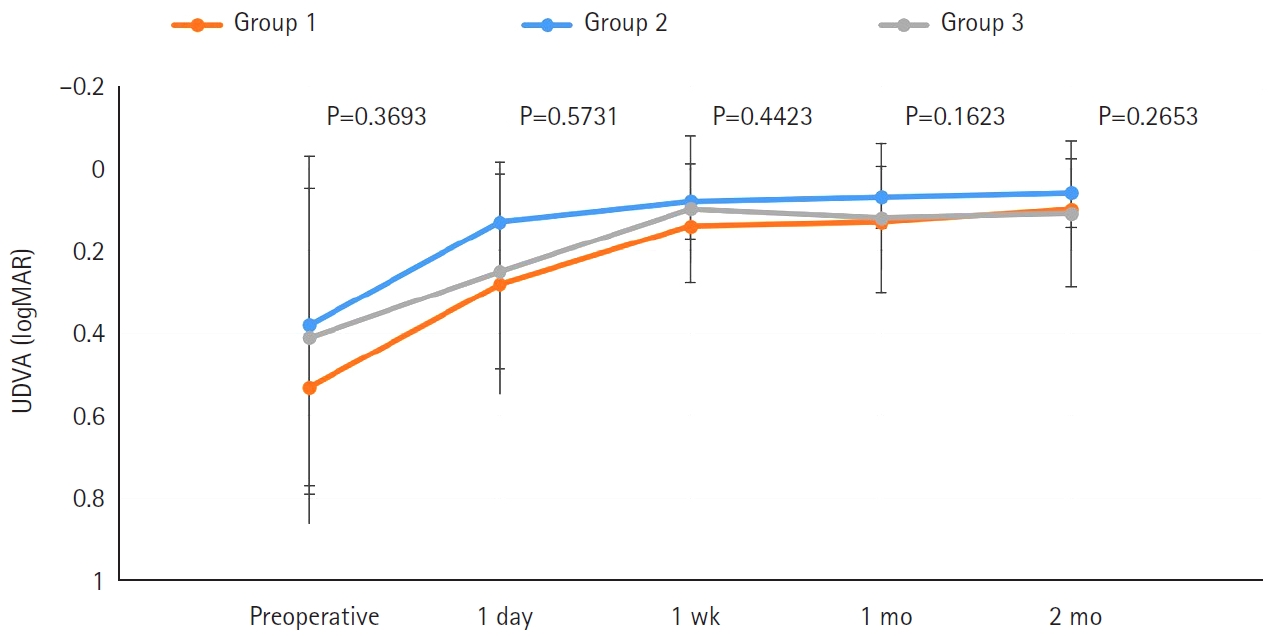
Fig. 2.Postoperative uncorrected intermediate visual acuity (UIVA) in patients with retinal disease who were treated using the three intraocular lenses. The postoperative UIVA in groups 1 and 2 was better than that in group 3 (P<0.05). Group 1: enhanced monofocal ICB00, n=36; Group 2: extended depth of focus ZXR00, n=36; Group 3: monofocal ZCB00, n=31. *P<0.05.
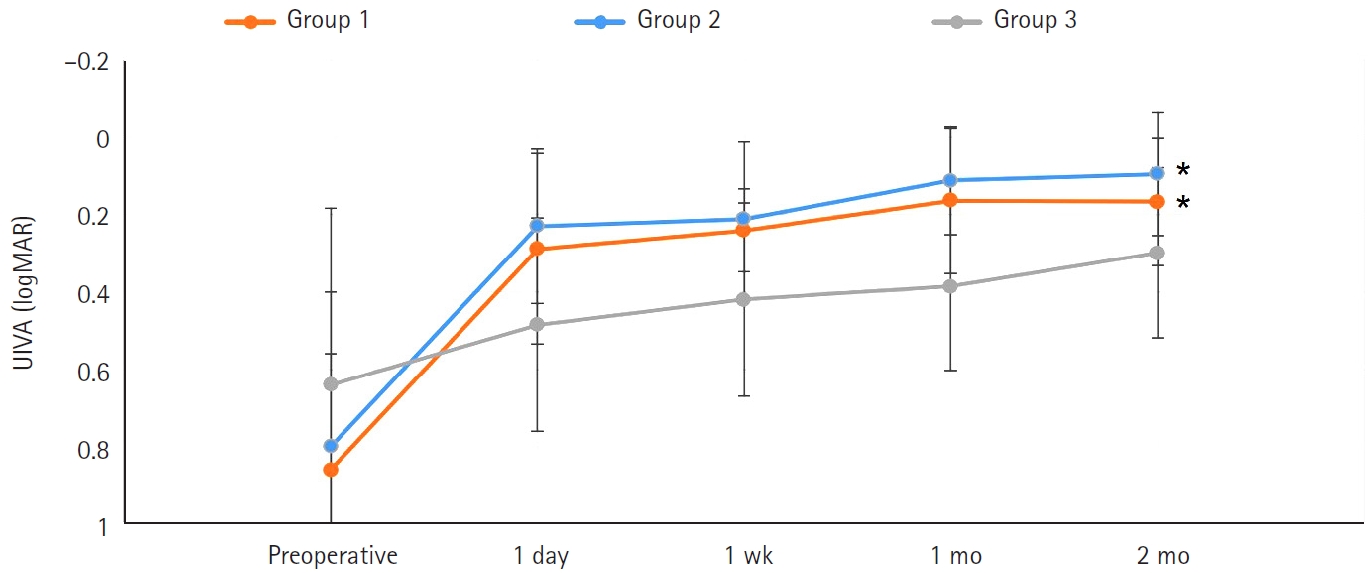
Fig. 3.Postoperative uncorrected near visual acuity (UNVA) in patients with retinal disease who were treated using the three intraocular lenses. The postoperative UNVA in group 2 was better than that in groups 1 and 3 (P<0.05). Group 1: enhanced monofocal ICB00, n=36; Group 2: extended depth of focus ZXR00, n=36; Group 3: monofocal ZCB00, n=31.
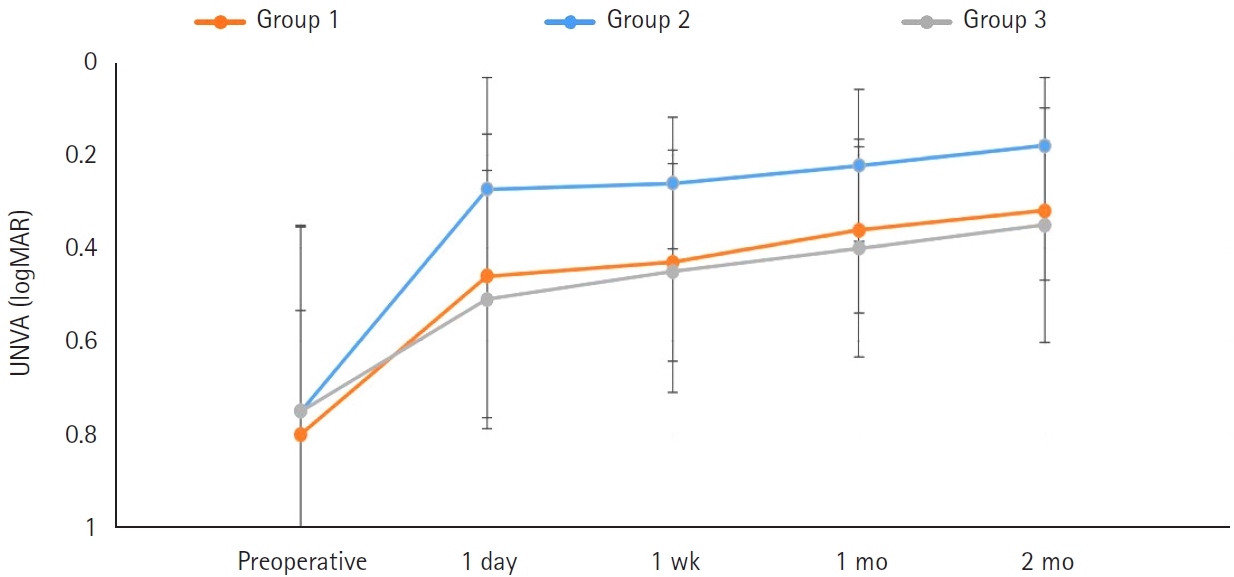
Fig. 4.Mean defocus curves of the three intraocular lens groups. Groups 1 and 2 exhibited significantly better defocus results at defocus ranges of –1.5 and –2 D (corresponding to 67–50 cm) than group 3 (P<0.05). Group 2 showed significantly better defocus results at a defocus range of –3 D (corresponding to 33 cm) than groups 1 and 3 (P<0.05). Group 1: enhanced monofocal ICB00, n=36; Group 2: extended depth of focus ZXR00, n=36; Group 3: monofocal ZCB00, n=31. *P<0.05.
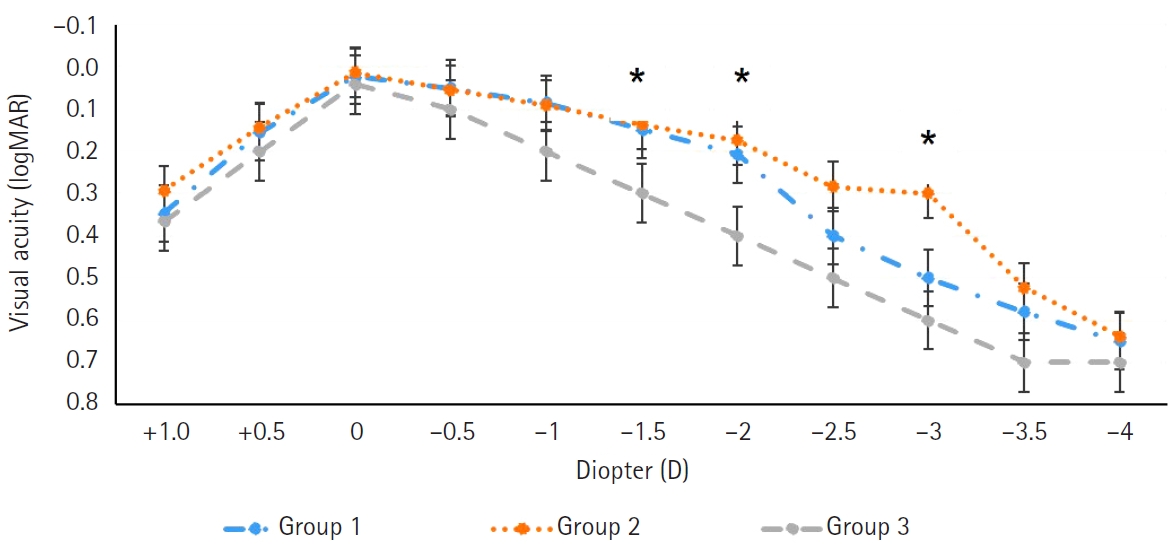
Fig. 5.Postoperative uncorrected distance visual acuity (UDVA) of the three intraocular lens groups according to the diagnosed retinal disease. The UDVA of patients with macular edema and macular holes was non-significantly lower than that of patients with epiretinal membranes and high myopia. POD, postoperative day. Group 1: enhanced monofocal ICB00, n=36; Group 2: extended depth of focus ZXR00, n=36; Group 3: monofocal ZCB00, n=31.

Table 1.Preoperative data of patients
| Parameter | Group 1a) | Group 2 | Group 3 |
|---|---|---|---|
| Age (yr) | 64.2±8.4 (45–75) | 61.4±9.1 (36–76) | 61.4±9.1 (47–82) |
| MRSE (D) | –1.72±2.91 (–2.15 to +1.25) | –0.70±2.64 (–2.38 to +0.75) | 0.75±2.24 (–1.30 to +1.50) |
| UDVA (logMAR) | 0.53±0.33 (0.15 to 0.81) | 0.38±0.41 (0.00 to 1.00) | 0.41±0.36 (0.05 to 1.00) |
| CDVA (logMAR) | 0.31±0.27 (0.1 to 0.6) | 0.25±0.23 (0.15 to 0.7) | 0.30±0.25 (0.1 to 0.6) |
| Eye | 36 | 36 | 31 |
Values are presented as mean±standard deviation (range). There was no statistically significant difference between the three groups (P>0.05).
MRSE, manifest refraction spherical equivalent; D, diopter; UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; logMAR, logarithm of the minimum angle of resolution.
a)Group 1, enhanced monofocal ICB00; Group 2, extended depth of focus ZXR00; Group 3, monofocal ZCB00.
Table 2.Postoperative outcomes at 2 months after surgery
| Parameter | Group 1a) | Group 2 | Group 3 |
|---|---|---|---|
| UDVA (logMAR) | 0.15±0.13 (0 to 0.3) | 0.12±0.14 (0 to 0.3) | 0.16±0.14 (0 to 0.3) |
| CDVA (logMAR) | 0.03±0.02 (0 to 0.15) | 0.04±0.03 (0 to 0.09) | 0.04±0.02 (0 to 0.09) |
| UIVA (logMAR) | 0.13±0.12 (0 to 0.3)* | 0.10±0.11 (0 to 0.3)* | 0.25±0.15 (0 to 0.4) |
| UNVA (logMAR) | 0.32±0.20 (0.1 to 0.52) | 0.18±0.12 (0 to 0.40)* | 0.45±0.26 (0.30 to 0.70)* |
| MRSE (D) | –0.28±0.24 (–1.00 to 1.50) | –0.32±0.29 (–1.25 to 1.25) | –0.35±0.26 (–1.25 to 1.25) |
| Eye | 36 | 36 | 31 |
Values are presented as mean±standard deviation (range). The UNVA was significantly better in group 2 than in groups 1 and 3.
UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; UIVA, uncorrected intermediate visual acuity; UNVA, uncorrected near visual acuity; logMAR, logarithm of the minimum angle of resolution; MRSE, manifest refraction spherical equivalent; D, diopter.
a)Group 1, enhanced monofocal ICB00; Group 2, extended depth of focus ZXR00; Group 3, monofocal ZCB00.
*P<0.05.
Table 3.Subjective satisfaction scores
| Parameter | Group 1a) | Group 2 | Group 3 |
|---|---|---|---|
| Overall satisfaction | 1.58±0.81* | 1.46±0.75* | 1.83±0.97 |
| Far vision satisfaction | 1.43±0.79 | 1.53±1.02 | 1.38±0.75 |
| Near vision satisfaction | 1.84±1.11 | 1.59±1.03* | 2.36±1.58 |
| Glare, halo | 1.59±1.07* | 2.21±1.16 | 1.51±1.06* |
| Eye | 36 | 36 | 31 |
Values are presented as mean±standard deviation. Low score means high satisfaction. The overall vision satisfaction was significantly higher in groups 1 and 2 than in group 3 (P<0.05). The near vision satisfaction was significantly higher in groups 1 and 2 than in group 3 (P<0.05). The glare and halo scores in group 1 and 3 were significantly lower than those in groups 2 (P<0.05).
a)Group 1, enhanced monofocal ICB00; Group 2, extended depth of focus ZXR00; Group 3, monofocal ZCB00.
*P<0.05.
- 1. de Silva SR, Evans JR, Kirthi V, et al. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev 2016;12:CD003169.ArticlePubMed
- 2. Braga-Mele R, Chang D, Dewey S, et al; ASCRS Cataract Clinical Committee. Multifocal intraocular lenses: relative indications and contraindications for implantation. J Cataract Refract Surg 2014;40:313‒22. ArticlePubMed
- 3. Chang JS, Ng JC, Lau SY. Visual outcomes and patient satisfaction after presbyopic lens exchange with a diffractive multifocal intraocular lens. J Refract Surg 2012;28:468‒74. ArticlePubMed
- 4. MacRae S, Holladay JT, Glasser A, et al. Special report: American Academy of Ophthalmology Task Force consensus statement for extended depth of focus intraocular lenses. Ophthalmology 2017;124:139‒41. ArticlePubMed
- 5. Cochener B. Clinical outcomes of a new extended range of vision intraocular lens: International Multicenter Concerto Study. J Cataract Refract Surg 2016;42:1268‒75. ArticlePubMed
- 6. Pandit RT. Monocular clinical outcomes and range of near vision following cataract surgery with implantation of an extended depth of focus intraocular lens. J Ophthalmol 2018;2018:8205824.ArticlePubMedPMCPDF
- 7. Kohnen T, Böhm M, Hemkeppler E, et al. Visual performance of an extended depth of focus intraocular lens for treatment selection. Eye (Lond) 2019;33:1556‒63. ArticlePubMedPMCPDF
- 8. Pedrotti E, Bruni E, Bonacci E, et al. Comparative analysis of the clinical outcomes with a monofocal and an extended range of vision intraocular lens. J Refract Surg 2016;32:436‒42. ArticlePubMed
- 9. Monaco G, Gari M, Di Censo F, et al. Visual performance after bilateral implantation of 2 new presbyopia-correcting intraocular lenses: trifocal versus extended range of vision. J Cataract Refract Surg 2017;43:737‒47. ArticlePubMed
- 10. Ruiz-Mesa R, Abengózar-Vela A, Aramburu A, Ruiz-Santos M. Comparison of visual outcomes after bilateral implantation of extended range of vision and trifocal intraocular lenses. Eur J Ophthalmol 2017;27:460‒5. ArticlePubMedPDF
- 11. Unsal U, Sabur H. Comparison of new monofocal innovative and standard monofocal intraocular lens after phacoemulsification. Int Ophthalmol 2021;41:273‒82. ArticlePubMedPDF
- 12. Shetty N, Shetty R, Ranade R, et al. Using adaptive optics to optimize the spherical aberration of eyes implanted with EDOF and enhanced monofocal intraocular lenses. J Cataract Refract Surg 2024;50:30‒6. ArticlePubMed
- 13. Alió JL, Plaza-Puche AB, Piñero DP, et al. Quality of life evaluation after implantation of 2 multifocal intraocular lens models and a monofocal model. J Cataract Refract Surg 2011;37:638‒48. ArticlePubMed
- 14. Grzybowski A, Kanclerz P, Tuuminen R. Multifocal intraocular lenses and retinal diseases. Graefes Arch Clin Exp Ophthalmol 2020;258:805‒13. ArticlePubMedPMCPDF
- 15. Zeng M, Liu Y, Liu X, et al. Aberration and contrast sensitivity comparison of aspherical and monofocal and multifocal intraocular lens eyes. Clin Exp Ophthalmol 2007;35:355‒60. ArticlePubMed
- 16. Kamath GG, Prasad S, Danson A, Phillips RP. Visual outcome with the array multifocal intraocular lens in patients with concurrent eye disease. J Cataract Refract Surg 2000;26:576‒81. ArticlePubMed
- 17. Jeon S, Choi A, Kwon H. Clinical outcomes after implantation of extended depth-of-focus AcrySof® Vivity® intraocular lens in eyes with low-grade epiretinal membrane. Graefes Arch Clin Exp Ophthalmol 2022;260:3883‒8. ArticlePubMedPDF
- 18. Grzybowski A, Kanclerz P, Muzyka-Woźniak M. Methods for evaluating quality of life and vision in patients undergoing lens refractive surgery. Graefes Arch Clin Exp Ophthalmol 2019;257:1091‒9. ArticlePubMedPDF
- 19. Jeon YJ, Yoon Y, Kim TI, Koh K. Comparison between an intraocular lens with extended depth of focus (Tecnis Symfony ZXR00) and a new monofocal intraocular lens with enhanced intermediate vision (Tecnis Eyhance ICB00). Asia Pac J Ophthalmol (Phila) 2021;10:542‒7. ArticlePubMedPMC
References
Figure & Data
References
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteEfficacy of extended depth of focus, enhanced monofocal, and monofocal intraocular lenses in patients with retinal disease
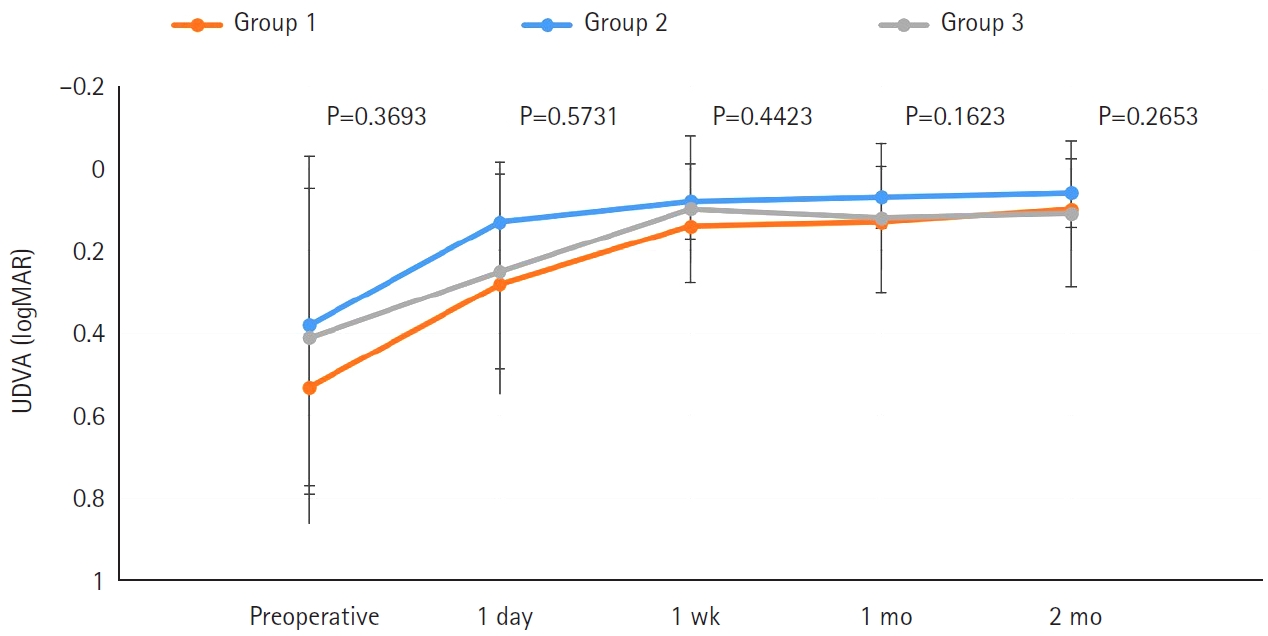
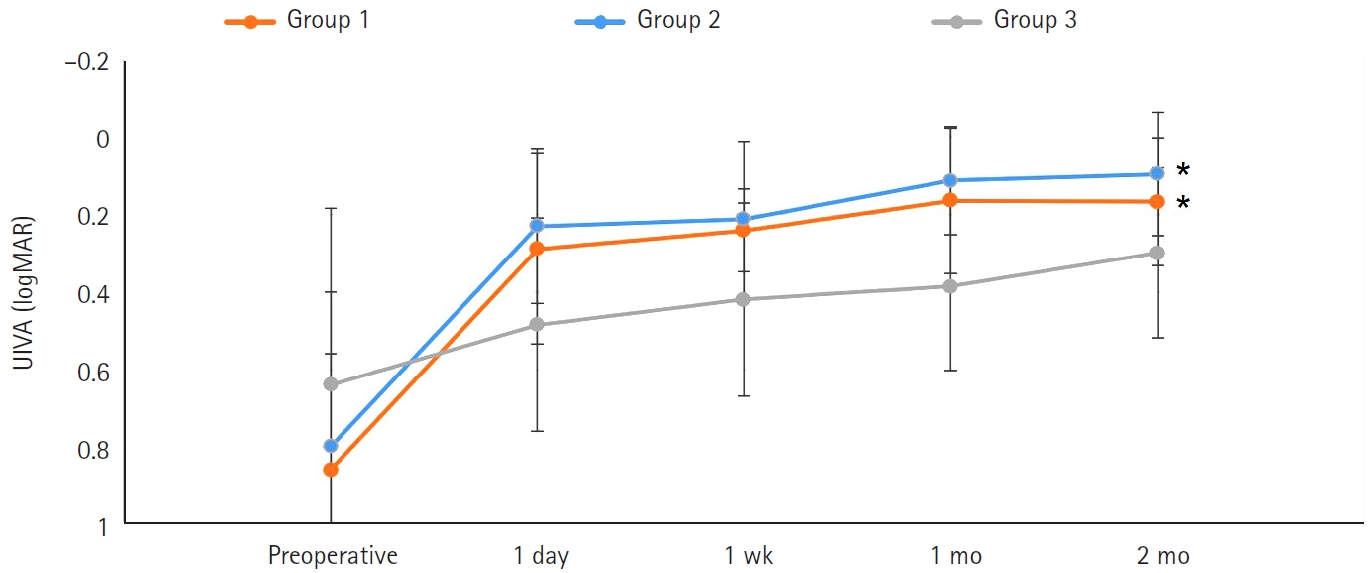
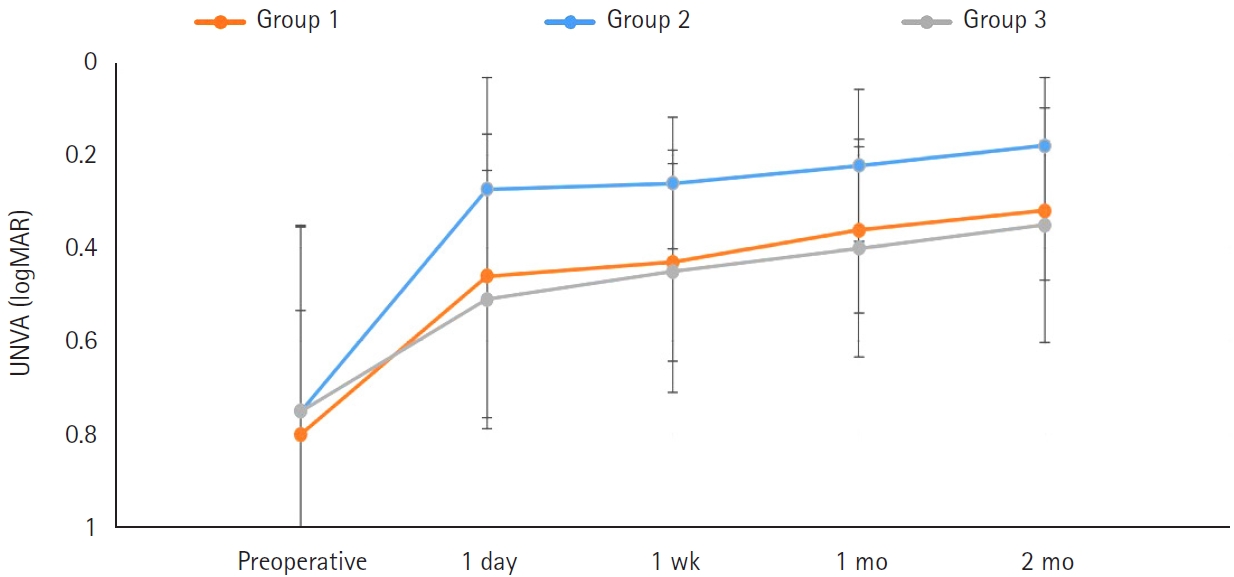
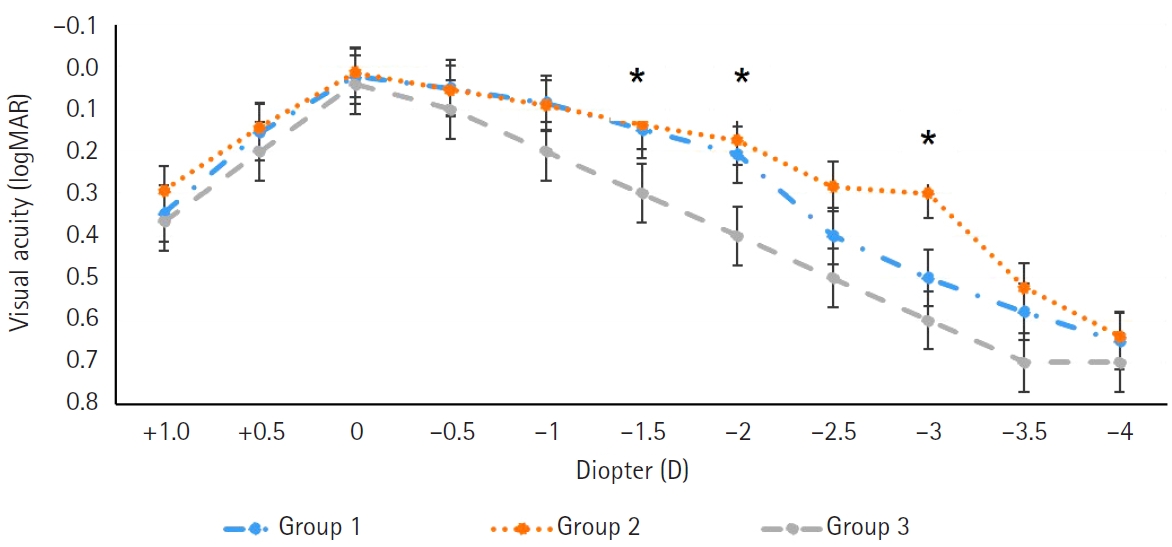

Fig. 1. Postoperative uncorrected distance visual acuity (UDVA) in patients with retinal disease who were treated using the three intraocular lenses. The postoperative UDVA values in the three groups were better than the preoperative values, respectively (P<0.05). However, there was no statistically significant difference in postoperative UDVA among the three groups. Group 1: enhanced monofocal ICB00, n=36; Group 2: extended depth of focus ZXR00, n=36; Group 3: monofocal ZCB00, n=31.
Fig. 2. Postoperative uncorrected intermediate visual acuity (UIVA) in patients with retinal disease who were treated using the three intraocular lenses. The postoperative UIVA in groups 1 and 2 was better than that in group 3 (P<0.05). Group 1: enhanced monofocal ICB00, n=36; Group 2: extended depth of focus ZXR00, n=36; Group 3: monofocal ZCB00, n=31. *P<0.05.
Fig. 3. Postoperative uncorrected near visual acuity (UNVA) in patients with retinal disease who were treated using the three intraocular lenses. The postoperative UNVA in group 2 was better than that in groups 1 and 3 (P<0.05). Group 1: enhanced monofocal ICB00, n=36; Group 2: extended depth of focus ZXR00, n=36; Group 3: monofocal ZCB00, n=31.
Fig. 4. Mean defocus curves of the three intraocular lens groups. Groups 1 and 2 exhibited significantly better defocus results at defocus ranges of –1.5 and –2 D (corresponding to 67–50 cm) than group 3 (P<0.05). Group 2 showed significantly better defocus results at a defocus range of –3 D (corresponding to 33 cm) than groups 1 and 3 (P<0.05). Group 1: enhanced monofocal ICB00, n=36; Group 2: extended depth of focus ZXR00, n=36; Group 3: monofocal ZCB00, n=31. *P<0.05.
Fig. 5. Postoperative uncorrected distance visual acuity (UDVA) of the three intraocular lens groups according to the diagnosed retinal disease. The UDVA of patients with macular edema and macular holes was non-significantly lower than that of patients with epiretinal membranes and high myopia. POD, postoperative day. Group 1: enhanced monofocal ICB00, n=36; Group 2: extended depth of focus ZXR00, n=36; Group 3: monofocal ZCB00, n=31.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Efficacy of extended depth of focus, enhanced monofocal, and monofocal intraocular lenses in patients with retinal disease
| Parameter | Group 1 |
Group 2 | Group 3 |
|---|---|---|---|
| Age (yr) | 64.2±8.4 (45–75) | 61.4±9.1 (36–76) | 61.4±9.1 (47–82) |
| MRSE (D) | –1.72±2.91 (–2.15 to +1.25) | –0.70±2.64 (–2.38 to +0.75) | 0.75±2.24 (–1.30 to +1.50) |
| UDVA (logMAR) | 0.53±0.33 (0.15 to 0.81) | 0.38±0.41 (0.00 to 1.00) | 0.41±0.36 (0.05 to 1.00) |
| CDVA (logMAR) | 0.31±0.27 (0.1 to 0.6) | 0.25±0.23 (0.15 to 0.7) | 0.30±0.25 (0.1 to 0.6) |
| Eye | 36 | 36 | 31 |
| Parameter | Group 1 |
Group 2 | Group 3 |
|---|---|---|---|
| UDVA (logMAR) | 0.15±0.13 (0 to 0.3) | 0.12±0.14 (0 to 0.3) | 0.16±0.14 (0 to 0.3) |
| CDVA (logMAR) | 0.03±0.02 (0 to 0.15) | 0.04±0.03 (0 to 0.09) | 0.04±0.02 (0 to 0.09) |
| UIVA (logMAR) | 0.13±0.12 (0 to 0.3) |
0.10±0.11 (0 to 0.3) |
0.25±0.15 (0 to 0.4) |
| UNVA (logMAR) | 0.32±0.20 (0.1 to 0.52) | 0.18±0.12 (0 to 0.40) |
0.45±0.26 (0.30 to 0.70) |
| MRSE (D) | –0.28±0.24 (–1.00 to 1.50) | –0.32±0.29 (–1.25 to 1.25) | –0.35±0.26 (–1.25 to 1.25) |
| Eye | 36 | 36 | 31 |
| Parameter | Group 1 |
Group 2 | Group 3 |
|---|---|---|---|
| Overall satisfaction | 1.58±0.81 |
1.46±0.75 |
1.83±0.97 |
| Far vision satisfaction | 1.43±0.79 | 1.53±1.02 | 1.38±0.75 |
| Near vision satisfaction | 1.84±1.11 | 1.59±1.03 |
2.36±1.58 |
| Glare, halo | 1.59±1.07 |
2.21±1.16 | 1.51±1.06 |
| Eye | 36 | 36 | 31 |
Table 1. Preoperative data of patients
Values are presented as mean±standard deviation (range). There was no statistically significant difference between the three groups (P>0.05). MRSE, manifest refraction spherical equivalent; D, diopter; UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; logMAR, logarithm of the minimum angle of resolution. Group 1, enhanced monofocal ICB00; Group 2, extended depth of focus ZXR00; Group 3, monofocal ZCB00.
Table 2. Postoperative outcomes at 2 months after surgery
Values are presented as mean±standard deviation (range). The UNVA was significantly better in group 2 than in groups 1 and 3. UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; UIVA, uncorrected intermediate visual acuity; UNVA, uncorrected near visual acuity; logMAR, logarithm of the minimum angle of resolution; MRSE, manifest refraction spherical equivalent; D, diopter. Group 1, enhanced monofocal ICB00; Group 2, extended depth of focus ZXR00; Group 3, monofocal ZCB00. P<0.05.
Table 3. Subjective satisfaction scores
Values are presented as mean±standard deviation. Low score means high satisfaction. The overall vision satisfaction was significantly higher in groups 1 and 2 than in group 3 (P<0.05). The near vision satisfaction was significantly higher in groups 1 and 2 than in group 3 (P<0.05). The glare and halo scores in group 1 and 3 were significantly lower than those in groups 2 (P<0.05). Group 1, enhanced monofocal ICB00; Group 2, extended depth of focus ZXR00; Group 3, monofocal ZCB00. P<0.05.

